
Pain is a universally
understood sign of disease and the most common symptom bringing people to seek
medical attention. The International Association for the Study of Pain defines
pain as "an unpleasant sensory and emotional experience" associated
with actual or potential tissue damage. It is possible to describe different
types of pain, and they tend to present differently. The history and physical
examination help to identify these differences. Precise and systematic pain
assessment is required to make the correct diagnosis and thus establish the
most efficacious treatment plan for patients presenting with pain.
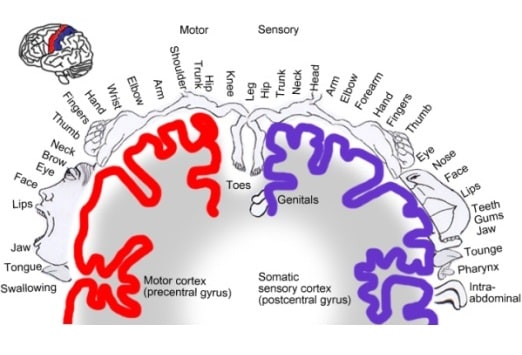
The somatosensory system (shown) is the part of the sensory
system concerned with the conscious perception of touch, pressure, pain,
temperature, position, movement, and vibration arising from the muscles,
joints, skin, and fascia. It is a 3-neuron system that relays sensations
detected in the periphery and conveys them via pathways through the spinal
cord, brainstem, and thalamic relay nuclei to the sensory cortex in the
parietal lobe. Impulses are carried from receptors via sensory afferents to the
dorsal root ganglia, where the cell bodies of the first-order neurons are
located. Their axons then travel through the spinal cord either in an
ipsilateral or a contralateral fashion. Second-order neuron cell bodies are
located in different anatomical areas depending on the sensation they carry.

The two major categories of pain are nociceptive and
neuropathic. This colonoscopy image demonstrates severe colitis that induced
visceral nociceptive pain. Nociception is a normal physiologic response to
stimuli, initiated by nociceptors that detect mechanical, thermal, or chemical
changes. It may be divided into three subtypes. Superficial somatic pain is
from cutaneous nociceptors on the skin or superficial tissues. Deep somatic
pain is from somatic nociceptors on ligaments, bones, blood vessels, and
muscles. Visceral pain is from visceral nociceptors within body organs.

Neuropathic pain is pain induced by damage to the nerves
themselves. Herpes zoster (shown) can cause neuropathic pain via growth and
inflammation within dermatomal nerves. Hyperpathic symptoms of burning,
tingling, or electrical sensations are classic for neuropathic pain.
Unfortunately, neuropathic pain is not traditionally responsive to standard
pain medications.

Sensitization is an adaptive process in which innocuous
stimuli produce an excessive response. Repeated intense stimuli to damaged
tissue lower the threshold and frequency of firing of afferent nociceptors.
Local inflammatory mediators contribute by recruiting additional nociceptors,
which normally remain silent to routine stimuli. For example, patients with bad
sunburns will experience severe pain and discomfort to even very light touches
because of sensitization of the pain fibers. Sensitization may also be partly
responsible in patients with chronic pain syndromes.
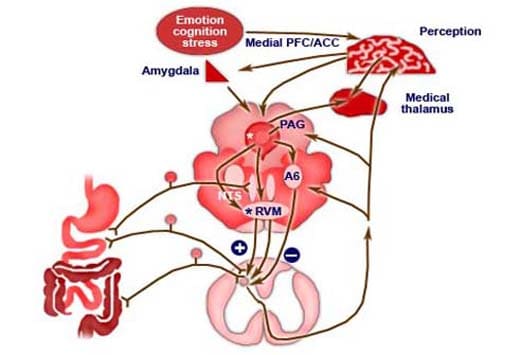
This image demonstrates the visceral afferent and modulatory
pathways responsible for the pain felt by patients with irritable bowel
syndrome. The plus sign denotes pain facilitation and the minus sign denotes
pain inhibition. Pain modulation can both enhance and dampen pain signals.
Placebo can have a significant analgesic response, and anxiety can magnify the
perceived stimuli. Descending signals from the frontal cortex and hypothalamus
help modulate the ascending transmission of the pain signal by opiate
receptors. (Abbreviations: A6, locus coeruleus; ACC, anterior cingulate cortex;
NTS, nucleus tractus solitarius; PAG, periaqueductal gray matter; PFC,
prefrontal cortex; RVM, rostra ventral medulla.)
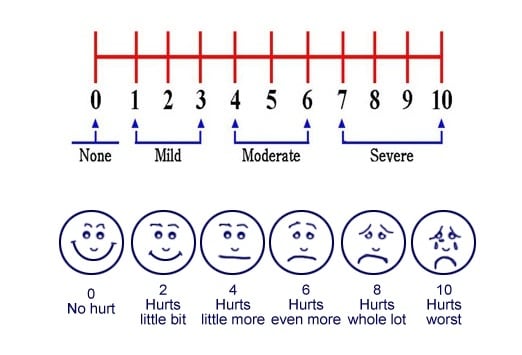
Determining the best treatment course for pain management
begins with identification of the intensity and duration of pain. Pain
assessment relies largely upon the use of self-report. Both single-dimensional
(rating only pain intensity) and multidimensional scales are available.
Examples of single-dimensional scales include the Numeric Rating Scale (top)
and the Wong-Baker Faces Pain Rating Scale (bottom).[2]Multidimensional
scales, such as the McGill Pain Questionnaire and the Brief Pain Inventory,
measure the intensity, the nature and location of the pain, and in some cases,
the impact the pain is having on activity or mood. The results obtained from
these instruments must be viewed as guides and not absolutes. Image courtesy of
the US Department of Veterans Affairs.

Laboratory tests, imaging, and nerve or muscle conduction
studies may help identify the root cause of a patient's pain, as well as
provide important information about therapeutic planning. For example, the
magnetic resonance imaging of a patient with cervical radiculopathy shown here
demonstrates a C6-7 disk herniation that is responsible for the patient's pain
symptoms. Depending on the extent of the injury, patients may be eligible for
injury-specific procedural interventions.
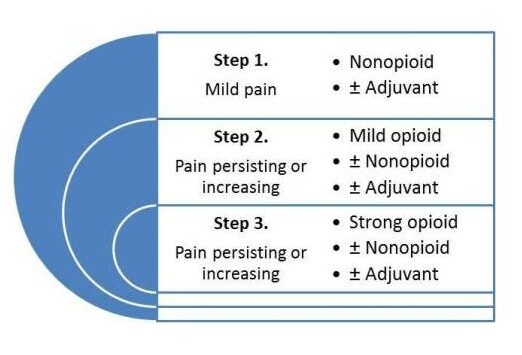
Medical management of pain proceeds in a stepwise fashion,
as shown here (based on the "pain ladder" by the World Health
Organization). Acute pain is typically treated with short courses of medication
therapy, whereas chronic pain may require long-acting medications or other
interventional modalities. For mild to moderate pain, nonnarcotic analgesics
are used, such as aspirin, acetaminophen, ibuprofen, naproxen, indomethacin,
ketorolac, and celecoxib. For moderate to severe pain, narcotic regimens are
typically used, including codeine, oxycodone, morphine, hydromorphone,
methadone, meperidine, fentanyl, and tramadol. Combination regimens that
contain opioids and nonnarcotic analgesics provide additive pain control.
Adjuvant medications therapies include tricyclic antidepressants,
antihistamines, and anticholinergics.

The pharmacology of pain control is based on influencing one
of several biochemical pathways. Many nonnarcotic analgesics inhibit the
cyclooxygenase enzyme, which is responsible for the formation of prostaglandin,
prostacyclin, and thromboxane. Opiate medications mimic endogenous opioid
peptides. Opioids bind to one of three principle classes of opioid receptors
(mu, kappa, delta) to produce centrally mediated analgesia. Tricyclic
antidepressants are thought to potentiate the effect of opiates. Image courtesy
of Wikimedia Commons.
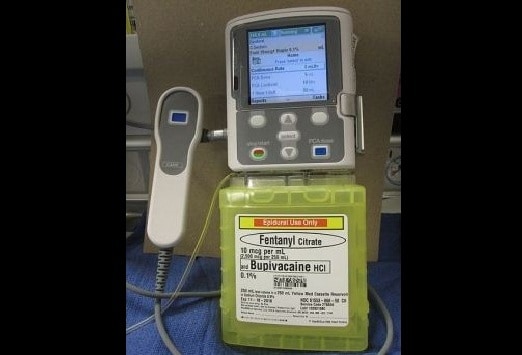
Patient-controlled analgesia allows patients to self-titrate
their intravenous pain medication. It allows for a more consistent administration
of analgesia with a reduced duration between when the patient feels pain and
when analgesia is administered. It reduces the chances for medication errors,
reduces nursing workload, increases patient autonomy, and provides objective
data about the amount of medication a patient needs. It is traditionally used
for postoperative patients and those with serious oncologic or hematologic
diseases. Image courtesy of Wikimedia Commons.

Transdermal patches provide controlled drug delivery with a
lower potential for abuse than oral analgesics. Patches can be applied once
every 12 to 24 hours. Conditions such as postherpetic neuralgia and chronic
cancer pain are routinely treated with transdermal patches. Opiate-infused
lollipops (shown) and buccal lozenges are other alternative forms of drug delivery
used to treat patients with malignant pain. Image courtesy of Wikimedia
Commons.

This patient is undergoing a sural nerve block. Regional
blocks with therapeutic injections can provide excellent relief for patients
with localized pain and inflammation. Depending on the clinical scenario,
therapeutic, sympathetic, diagnostic, prognostic, or prophylactic blocks may be
used. Therapeutic injections allow for a return to normal function, preventing
the development of compensatory injuries. The exact procedural technique is
dependent on the nerve involved, but the general principle involves the direct
injection of local anesthetic or corticosteroid into the perineural space.
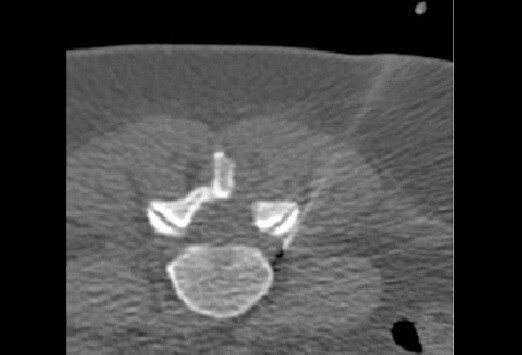
Depending on operator familiarity and the difficulty of
accessing injection sites, image guidance may be used for direct visualization.
This computed tomography-guided image demonstrates an injection needle in good
position in the outer aspect of the neural foramen. Computed tomography,
ultrasound, or fluoroscopic guidance allows for more precise needle placement,
thus reducing the amount of injected drug and reducing complications. The
procedure is especially useful in patients with distorted native anatomy.
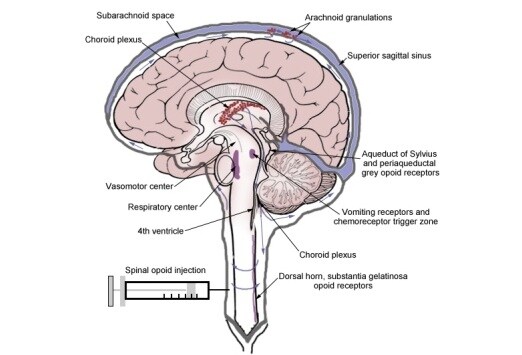
Surgical interventions are limited for patients with
discrete deficits who fail conservative management. Depending on the location
of pain, patients will typically undergo a stepwise treatment course involving
noninterventional management before being eligible for invasive therapy.
Surgically implanted devices, such as intrathecal pumps and spinal cord
stimulators, are available for use on a case-by-case basis. This image shows
the spread of opioids in the cerebrospinal fluid via a spinal injection. The
rostral spread of intrathecal opioids is thought to be responsible for unwanted
effects such as respiratory depression, pruritus, hypotension, nausea, and
vomiting. Image courtesy of Wikimedia Commons.

Spinal cord stimulation (SCS, shown) is approved by the FDA
for indications including failed back surgery syndrome, chronic painful
peripheral neuropathy, multiple sclerosis, complex regional pain syndromes,
ostherpetic neuralgia, post-thoracotomy pain, phantom limb pain, intercostal
neuralgia, and certain spinal cord injuries. The neurophysiologic mechanisms of
SCS are not completely understood. Experimental evidence supports a beneficial
SCS effect at the dorsal horn level, whereby the hyperexcitability of
wide-dynamic-range neurons is suppressed. Evidence exists for increased levels
of GABA release and serotonin and, perhaps, for reduced levels of some
excitatory amino acids, such as glutamate and aspartame. Image courtesy of
Wikimedia Commons.
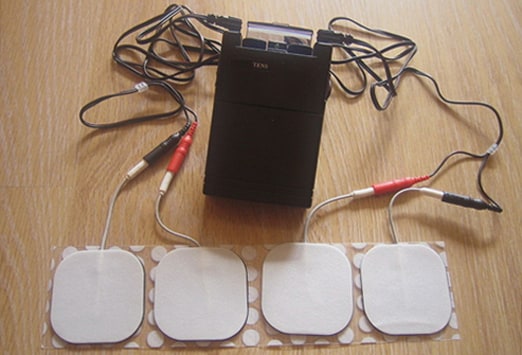
Transcutaneous electrical nerve stimulation (TENS) units are
adjuvant pain control devices that provide pulsatile electric impulses. The
proposed mechanisms by which they reduce pain are presynaptic signal
inhibition, endogenous pain control, direct inhibition of abnormally excited
nerves, and restoration of afferent inputs. TENS units have been used for low
back, arthritic, sympathetically mediated, neurogenic, visceral, and
postsurgical pain. Although they are widely used and there is a great deal of
anecdotal and observation-based evidence, there is a paucity of randomized
controlled trials confirming the effectiveness of TENS units. Image courtesy of
Wikimedia Commons.

Chronic, refractory pain is best managed with a
multidisciplinary team approach that includes psychology, occupational therapy,
physical therapy, vocational rehabilitation, and relaxation training. Patients
with chronic pain frequently seek complementary and alternative medicine
treatment options as well, including acupuncture (shown), dietary supplements,
and hypnosis. A 2012 meta-analysis of 29 randomized controlled trials (17,922
patients) found acupuncture to be superior to both sham acupuncture and standard
care for the treatment of different types of chronic pain, suggesting that the
effects of acupuncture are more than just placebo effect. Image courtesy of
Wikimedia Commons.
Hey
ReplyDeleteAbsolutely brilliant.
really helpful.
please also read my blog:
Regards
https://www.kentmskclinic.co.uk/ultrasound-guided-spinal-injections/